I recently read an research article on pelvic floor muscle assessment and I found interesting the following parts:
- The pelvic floor muscles (PFM) consist of approximately 70% slow-twitch (type 1) and 30% fast-twitch (type 2) muscle fibres (Gilpin et al, 1989).
- During a vaginal examination using the distal pad of the index finger to palpate the perivaginal muscles, a definite bulging and lifting of the muscles are felt during a contraction, and in both the contracted and relaxed state, areas of atrophy can be detected.
- A moderate to strong contraction of the levator ani muscles has both a squeeze and a lift component.
- Regarding different muscle components (that is, fast- and slow-twitch fibres), it has been shown that fast fibres are recruited only during activities involving speed and/or power (Edwards, 1978) and if the response to a command to contract the PFM maximally is sluggish, then it is probable that only slow-twitch muscle fibres are being used. Jones and Rutherford (1987) reported that in some untrained muscles, the fast-firing muscle fibres are never recruited, and so these may need targeting in some other way during PFM rehabilitation. Gosling et al (1981) described the PFM slow-twitch fibres as being responsible for maintaining continuous muscle activity over prolonged periods, with the fast-twitch fibres recruited reflexly during sudden increases in intra-abdominal pressure, for example when coughing. A reduction in slow-twitch activity would therefore manifest itself in a short duration contraction and few repetitions, and PFM in this category may thus be responsible for decreased support of the proximal urethra and reduced urethral occlusion. A reduction in fast-twitch fibre activity may result in a slower, weaker reflex response to increases in intra-abdominal pressure. Logically, one should assess both the fast- and slow-twitch muscle fibre activity before planning an exercise regimen.
- Exercise programme planning: the plethora of PFM exercise regimens in the literature indicates a lack of standardisation and, when compared with general rehabilitation methodology, the reports show lack of scientific application. There is a wide range of muscular strength and endurance across any female population, and so it is postulated that a uniform, standard regimen is not appropriate. Instead, assessment of the fast- and slow-twitch components, leading to an individual exercise programme, has been proposed, to target specifically the weakness of each individual patient.
- Muscle weakness leads to reduction in mitochondrial oxidative capacity as indicated by a decrease in the succinate dehydrogenase (SDH) activity (Eriksson and Haggmark, 1979). Consequently, these same authors maintain that it is necessary to gradually increase the SDH reserves by repeated contractions which will deplete levels and stimulate greater production. This reinforces the theory of overload and supports the need for a programme of regular daily contractions advanced in this study.
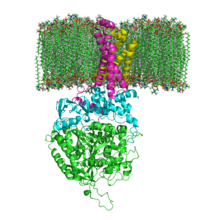
Interesting also to know that SDH or succinate-coenzyme Q reductase (SQR) or respiratory Complex II is an enzyme complex, bound to the inner mitochondrial membrane of mammalian mitochondria and many bacterial cells. It is the only enzyme that participates in both the citric acid cycle and the electron transport chain.
The fundamental role of SDH in the electron transfer chain of mitochondria makes it vital in most multicellular organisms, removal of this enzyme from the genome has also been shown to be lethal at the embryonic stage in mice. Mutations of different genes used in its construction can lead to:
- Leigh syndrome, mitochondrial encephalopathy, and optic atrophy
- Tumorogenesis in chromaffin cells, causing hereditary paraganglioma and hereditary pheochromocytoma. Tumors tend to be malignant. It can also lead to decreased life-span and increased production of superoxide ions.
- Decreased life-span, increased production of superoxide ions, hereditary paraganglioma and hereditary pheochromocytoma. Tumors tend to be benign. These mutations are uncommon.
- Hereditary paraganglioma and hereditary pheochromocytoma. Tumors tend to be benign, and occur often in the head and neck regions. These mutations can also decrease life-span and increase production of superoxide ions.
Mammilian succinate dehydrogenase functions not only in mitochondrial energy generation, but also has a role in oxygen sensing and tumor suppression; and, therefore, is the object of ongoing research.
No comments:
Post a Comment