This small cavity that appears at the radial side of the hand when we fully extend and abduct our thumb is call "anatomical snuff box" or "tabatiere anatomique".
The bony borders of this cavity are:
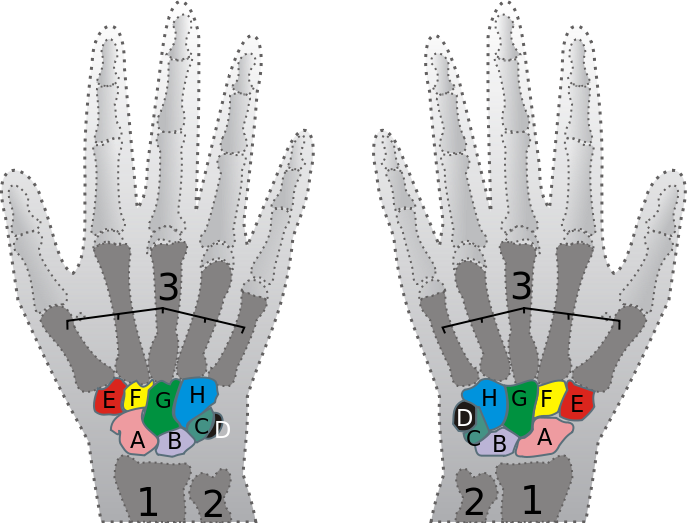
(bottom surface) the trapezium and scaphoideum
(proximally) the styloid process of the radius
(distally) the apex of the muscle tendons triangle
Three tendons define the borders of this cavity, as seen in the picture above:
1. Extensor pollicis longus
Origin: dorsal surface of the ulnar & the membrana interossea
Insertion: phalanx I (dorsally at the base of the distal phalanx)
Action: wrist: RAD DIV, EXT - thump: EXT at the metacarpophalangeal and the interphalangeal joints
While abductor pollicis brevis and adductor pollicis, both attached to the extensor pollicis longus tendon, can extend the thumb's interphalangeal joint to the neutral position, only extensor pollicis longus can achieve full hyperextension at the interphalangeal joint
Innervation: n. Radialis (C7-C8)
2. Extensor pollicis brevis
Origin: dorsal surface of the radius & the membrana interossea
Insertion: phalanx I (dorsally at the base of the proximal phalanx)
Action: wrist: RAD DIV - thump: EXT at the carpometacarpal and the metacarpophalangeal joints
Innervation: n. Radialis (C7-C8)
3. Abductor pollicis longus
Origin: dorsal surface of the ulnar & the radius & the membrana interossea
Insertion: base of the metacarpi I
Action: wrist: RAD DIV - thump: ABD at the carpometacarpal joint
Innervation: n. Radialis (C7-C8)
Besides, the
radial artery of the forearm passes through this cavity. It runs distally on the anterior part of the forearm. There, it serves as a landmark for the division between the anterior and posterior compartments of the forearm, with the posterior compartment beginning just lateral to the artery. The artery winds laterally around the wrist, passing through the anatomical snuff box and between the heads of the first dorsal interosseous muscle.
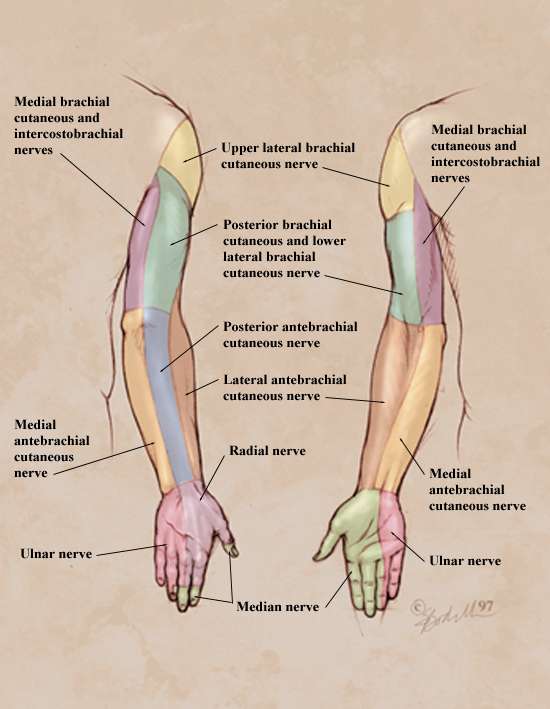
The dorsal (superficial) cutaneous branch of the radial nerve can be palpated by stroking along the extensor pollicis longus with the dorsal aspect of a fingernail.
Pathology
1. Scaphoideum fracture
In the event of a fall onto an outstretched hand, the articulation between the scaphoideum and the radius is the area through which the brunt of the force will focus. In case the force is big enough the scaphoideum may fracture. There are two anatomical peculiarities that make this fracture quite dangerous and difficult to treat:
a. The size of the scaphoideum - the scaphoid is a small, oddly shaped bone whose purpose is to facilitate mobility rather than confer stability to the wrist joint. In the event of inordinate application of force over the wrist, this small scaphoid is clearly likely to be the weak link.
b. The vascularization of the scaphoideum - blood enters the scaphoid distally. Consequently, in the event of a fracture the proximal segment of the scaphoid will be devoid of a vascular supply, and will - if action is not taken - avascularly necrose within a sufferer's snuffbox.
2. DeQuervain’s tenosynovitis
DeQuervain's tenosynovitis is an inflammation of the fluid-filled sheath (called the synovium) that surrounds the tendons of the muscles mentioned above. Mostly, the extensor pollicis brevis and the abductor pollicis longus are the muscles affected in that case. The main reason for this inflammation is overuse syndromes. The main symptoms are pain, tenderness, and swelling over the thumb side of the wrist, and difficulty gripping. The
Finkelstein's test may be positive.
3. Cheiralgia paresthetica
Cheiralgia paresthetica or Wartenberg's syndrome is the compression of the radial nerve along its course in the forearm. The area affected is typically on the back or side of the hand at the base of the thumb, near the anatomical snuffbox, but may extend up the back of the thumb and index finger and across the back of the hand. The most common cause is thought to be constriction of the wrist, as with a bracelet or watchband. Symptoms include numbness, tingling, burning or pain. Since the nerve branch is sensory there is no motor impairment.
There might be other injuries that can cause symptoms around the region as well like osteoarthritis, carpal instabilities, or cervical radiculopathy (C7-8). However, these were the 3 main problems that can appear and a Physical Therapist should at least be aware of in order to successfully assess a patient.